| A few years ago, I started putting in two Herbert screws for scaphoid fractures, with the thought that it would provide more rigid fixation. I think that it is helpful in some, but not all cases. Here are some of my results with a few variations... |
| Click on each image for a larger picture |
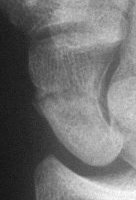
| 1. Nondisplaced fracture in a surgeon who declined continuous immobilization. |
 |
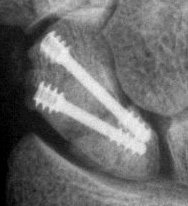
| One week after screw stabilization using a limited dorsal approach, he was back operating, but splinted when not scrubbed. These films are one month post op: no visible fracture. |
 |
 |
| Case 2. Nonunion with a large fracture cyst. After debridement, the defect, the graft, and yes, that is the capitate peeking through the defect. |
 |
 |
 |
| The graft, and inadequate seating of the more ulnar screw. |
 |
| Consolidation.. |
 |
 |
| The poorly placed screw remained a source of pain, and the hardware was removed along with a styloidectomy. |
 |
| Case 3. Another postop, better screw positioning. |
 |
| Case 4. Nonunion with a graft and screws placed in both directions from a single palmar approach, hyperextending the wrist for the proximal entry... |
 |
| and with the graft: |
 |
| and with consolidation, |
 |
 |
| Case 5. Another,same bidirectional
technique. Here, I ran the second screw too close to the first, and may
have flattened the leading threads - not
ideal. The preop status: |
 |
| With intercalated iliac bone graft... |
 |
| and healing. |
 |
 |
| Case 6. A dorsal approach for this proximal pole fracture would have been a better choice. |
 |
 |
 |
 |
| Case 7. This nonunion patient's scaphoid and iliac crest were unusually soft bone. |
 |
| After two screws, the fixation was
clearly inadequate, so I put a third screw through the graft into the proximal
pole. I wasn't sure whether to buy
stock in Herbert screws or Zantac. The fracture healed despite AWOL and no immobilization. |
 |
 |
| Case 8. Transscaphoid perilunate fracture dislocation... |
 |
 |
| Two screws put in dorsally, LT ligament reinforced with a strip of extensor retinaculum left attached to the triquetrium and anchored into the lunate; temporary capitolunate pin. |
 |
 |
| Late, with asymptomatic partial union or nonunion, but no haloing. |
 |
| Search for...
Herbert screw scaphoid |
Case Examples Index Page | e-Hand Home |